The World Health Organization declared SARS-CoV-2 a global pandemic on 11 March 2020. At the time, I was isolating at home after returning from CERN. I was not allowed on campus because I had been abroad when my university declared that all international travel for work purposes was ended.
But I never actually caught COVID-19, not then and not in the intervening 3 years. Catching it was inevitable, of course. The virus has mutated many times. It spreads and spreads. It’s reached a level at which it’s essentially endemic, taking its place alongside rhinovirus and influenza as a globe-trotting seasonal nuisance and/or killer. How can a human being in a global society avoid catching such a widespread disease?
And so, nearly 3 years to the day of the declaration of the global pandemic, I started feeling symptoms of a respiratory infection. It began on a Thursday night (March 9) with an urge to cough to clear my chest, and an urge to clear my throat. That never happens to me unless I am getting sick. I resolved to stay home the next day.
When I awoke on March 10, I knew I was worse and my decision to stay home was right. I worked from home and got tired a little more easily than usual that day, all while symptoms progressed: coughing, congestion, body aches, occasional chills. I never took my temperature, because I never felt feverish, but I wouldn’t be surprised if I was running at least a low-grade fever. That’s just a guess, though.
I did what everyone should do next: I took a COVID test. It was negative. But I also know that the rapid antigen tests rely on having a minimum viral load in the body to trigger the positive. A good scientist knows a single test is usually not a reliable measure of truth.
My symptoms reached the level of a bad rhinovirus or a mild-to-moderate flu. Given the negative COVID test, the most likely explanation was influenza. I was vaccinated for flu in the late fall and had the bivalent COVID vaccine in the early fall. But no vaccine is perfect; if the flu strains used to prepare that vaccine are mis-matched to those in circulation, it’s very possible to catch a case even if the symptoms are reduced. Still better than catching the disease while unprepared. A trained immune system is an effective immune system!
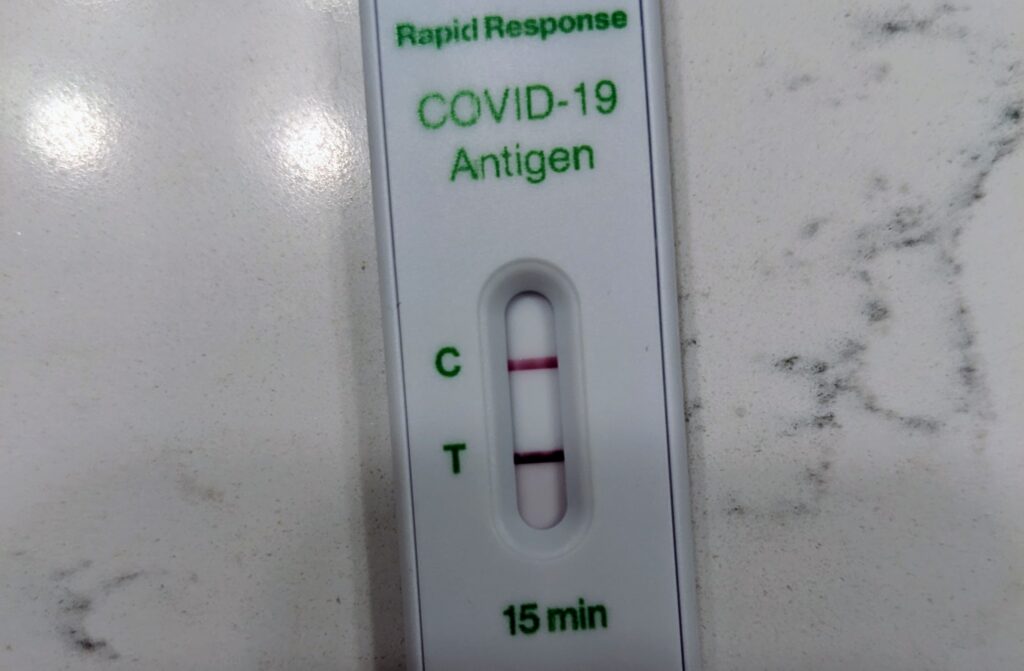
On Monday, I was compelled to test again. That evening, I took another rapid antigen test. It went positive so fast it was stunning. The “test” line was bold and thick and clear. The “control” line took several more moments to also appear. But it was undeniable: I was COVID-positive!
I’ve not really had any of the classic COVID symptoms, apart from a dry-ish cough. The loss of taste and/or smell did not happen, though I will admit I seem to be a lot more sensitive to spicy food and there was one meal where I could have sworn someone dumped an entire salt shaker in it. The sense of saltiness was intense … but the most likely explanation was that too much salt was, in fact, used in the dish.
I didn’t have any dramatic dropping of my blood oxygen level; a small portable pulse oxymeter reliably put by oxygen saturation levels at 97-98% or better. There was no high fever. I’ve definitely had flus worse than this, but not many colds worse than this. If anything, I would say that the respiratory symptoms – the coughing, the congestion, etc. – are hanging on longer than they would with either of those other two viral infections. Of course, it’s been 3+ years since I’ve had a serious infection, with only a minor cold once or twice in the last couple of years whose symptoms never lasted more than 48-72 hours. This one has hung on for a solid week.
Here, I get to statistically credit the vaccines. The best quality evidence is overwhelmingly in favor of COVID vaccination having a high probability of preventing severe COVID illness ((Ssentongo, P., Ssentongo, A.E., Voleti, N. et al. SARS-CoV-2 vaccine effectiveness against infection, symptomatic and severe COVID-19: a systematic review and meta-analysis. BMC Infect Dis 22, 439 (2022). https://doi.org/10.1186/s12879-022-07418-y)). For example, a review of studies whose scope includes 7 million individuals suggests that while the ability to fully prevent infection falls fast, even 5+ months after vaccination the probability of preventing the most severe illness is at the level of 90%. Certainly, I fall within that window for the time since my last vaccination, and this case has been mild. While a single case is not strong evidence of any one fact, this one fits well in the population of cases where severity has been reduced by vaccination.
At the time I write this, I am one week into my symptoms. They have declined in severity, but not disappeared. I no longer have to take decongestant or acetaminophen to be comfortable, which is nice. However, it’s clearly not done with me yet. This weekend, I will test again. If negative, I will wait 48 hours and test once more. If negative then, I will physically return to my workplace. However, if symptomatic (which at this pace I still expect to be) I will mask to the gills (plenty of N-95s still in our house!). The good thing about catching this so long after the start of the pandemic is that the process of managing oneself and protecting others from the disease are well-established, and simply need to be followed.
The only thing I wish were better were those rapid tests. Having better rapid tests that detect the virus much earlier in the symptomatic stage would be a huge benefit to society. If I had tested positive earlier, I might have taken additional precautions even in my own home. However, that was not possible … at least, not using a single test of this design.
Big picture: for COVID, this went well. Like flus and colds, I never want to get one again. But I WILL get this again, and I’d rather prepare before infection than suffer during infection. So I will keep following the best medical advice, which is to vaccinate and, if you get sick anyway, stay home and keep away from others to prevent the spread of disease, especially to those who cannot vaccinate but may be particularly vulnerable.